
Surgical Techniques for Rectal Prolapse

1
Department of Surgery, Gazi University School of Medicine, Ankara 06570, Turkey
2
Department of Proctology, Ankara Memorial Hospital, Ankara 06520, Turkey
3
Department of Surgery, Ankara Oncology Training and Research Hospital, Ankara 06200, Turkey
4
Department of Surgery, Ankara Yenimahalle Training and Research Hospital, Ankara 06170, Turkey
*
Author to whom correspondence should be addressed.
Gastroenterol. Insights 2021, 12(3), 310-318; https://doi.org/10.3390/gastroent12030028
Submission received: 8 May 2021
/
Revised: 2 June 2021
/
Accepted: 16 June 2021
/
Published: 1 July 2021
(This article belongs to the Special Issue Complete Rectal Prolapse: Etiopathogenesis, Diagnosis and Treatment)
{kind=link}
{kind=link}
{kind=link}
Abstract
:Complete rectal prolapse or rectal procidentia is a debilitating disease that presents with fecal incontinence, constipation, and rectal discharge. Definitive surgical techniques described for this disease include perineal procedures such as mucosectomy and rectosigmoidectomy, and abdominal procedures such as rectopexy with or without mesh and concomitant resection. The debate over these techniques regarding the lowest recurrence and morbidity rates, and the best functional outcomes for constipation or incontinence, has been going on for decades. The heterogeneity of available studies does not allow us to draw firm conclusions. This article aims to review the surgical techniques for complete rectal prolapse based on the current evidence base regarding surgical and functional outcomes.
1. Introduction
Complete rectal prolapse or rectal procidentia is defined as a full-thickness protrusion of the rectum through the anal canal, and should be distinguished from the mucosal prolapse [1]. Although the definite etiology of this disease is unclear, the most common related pathologies are the redundant sigmoid colon, a deep cul-de-sac, and the diastasis of levator ani muscles [2,3].
The incidence is higher in females, with a peak in the seventh decade [4]. Patients usually complain of fecal incontinence, which is thought to be a result of a chronic stretch of the anal sphincter and continuous stimulation of the rectoanal inhibitory reflex by the prolapsed tissue [5,6]. Other symptoms include constipation, pain, bloody or mucous rectal discharge [7].
The diagnosis can be made by demonstrating the protrusion of the rectal circumferential radial folds with straining maneuvers on clinical examination [7]. However, additional diagnostic tests such as dynamic pelvic magnetic resonance imaging (MRI), anal manometry, and endoanal ultrasonography (EUS) are usually required to detect co-existing anatomical abnormalities and decide on the optimal surgical treatment method [8,9,10,11,12].
Described surgical techniques are varied, and whether the approach is abdominal or perineal, the treatment aims to correct anatomical and functional abnormalities by the fixation of the rectum to the sacrum and/or the resection of the redundant bowel [13]. In this article, these different techniques are reviewed for their surgical and functional outcomes and explained in the technical notes section with figures based on our cases.
2. Surgical Techniques
As a general consideration, perineal procedures have been associated with reduced complication rates and chosen in frail patients with co-morbidities. However, with recent randomized controlled trials and reviews, perineal and abdominal procedures have been reported to have similar outcomes in expert hands regarding perioperative complications, recurrence rate, and quality of life [14].
A recent Cochrane Database review demonstrated no significant difference in recurrence rates [15], and Mustain et al. reported no difference in terms of postoperative complications between these two approaches [16]. Moreover, Emile et al. revealed that similar recurrence and complication rates were seen, but increased length of hospital stay in perineal procedures and longer operative time in abdominal procedures were noted [17].
2.1. Abdominal Approach
Described techniques, whether rectopexy using a mesh or suture and/or resection, have been proven to be effective and safe via laparoscopy [13]. The laparoscopic approach for rectal prolapse has been associated with shorter hospital stay and less postoperative pain. Moreover, there was no statistical difference in recurrence rates, postoperative constipation, or incontinence scores [18,19,20].
2.1.1. Ripstein Procedure (Anterior Mesh Rectopexy)
This procedure was first described by Ripstein in 1952 [21]. Reported results ranged from 0 to 13% for recurrence and 0 to 2.8% for mortality, with high complication rates of 33% [22]. Its well-recognized complication was the obstruction and narrowing of the rectum; therefore, patients may complain from newly developed or worsened constipation in the postoperative setting [23].
Laparoscopic anterior mesh rectopexy (LAMR) was reported to have 5.1% morbidity and 3% recurrence rates in a study including 175 consecutive patients [24]. In a review of 12 non-randomized studies, reporting low recurrence rates and favorable functional outcomes in long-term follow-up, LAMR is considered an efficient procedure for complete rectal prolapse [25].
Technical notes:
It requires complete rectal mobilization followed by placement of an anterior mesh, fixating the antimesenteric surface and sides of the rectum to the sacral promontory. To achieve a more accurate dissection plane, rectal mobilization should be started from the posterior to the lateral. The anterior mobilization is continued 2–3 cm into the Denonvilier’s fascia. The mesh should be placed in the lower rectum approximately 4–5 cm below the sacral promontory, which results in an anteriorly mesh-wrapped rectum. Then the mesh is fixed with 2-0 prolene sutures to the presacral fascia and to the antimesenteric surface of the rectum [21,26].
2.1.2. Wells Procedure (Posterior Mesh Rectopexy)
With the use of absorbable materials instead of non-absorbable materials, as initially described by Wells, recurrence and complicatons such as pelvic sepsis have been lower with posterior mesh rectopexy [27].
Laparoscopic posterior mesh rectopexy (LPMR) was investigated by several prospective studies [28,29,30]. Dyrberg et al. reported a recurrence rate of 11%, as well as improvements in continence and constipation scores (74% and 65%, respectively) [29]. In a comparative study with a mean follow-up of 46 months, recurrence rates were found to be 3%, and this was similar to the laparoscopic ventral mesh rectopexy (LVMR) group, whereas patients with LPMR had less improvement in constipation scores [31].
Technical notes:
Historically, an Ivalon sponge (non-absorbable) was used for wrapping around the fully mobilized rectum and then suturing it to the presacral fascia. Because of the high infection rates, this technique has been eventually modified with different meshes and partial mobilization of the rectum on the right and posterior side, which enabled suturing the mesh to the sacral promontory.
The rectal mobilization is performed in the mesorectal plane laterally and posteriorly, reaching the level of the pelvic floor, and the anterior dissection is kept limited. The mesh is placed in the mid-sacral level, fixated with 2/0 non-absorbable sutures to the presacral fascia, and a loose wrap of <270 around the rectum [32].
2.1.3. Suture Rectopexy
Suture rectopexy was first described by Cutait in 1959, and it aimed to form scar tissue between the rectum and sacrum [33,34]. Presumably, due to extensive rectal mobilization, postoperative constipation rates are increased [15,35].
Laparoscopic suture rectopexy (LSR) has been demonstrated as an efficient procedure for patients with prominent symptoms of incontinence [36,37]. Sahoo et al. revealed that LSR and LPMR have no difference regarding functional outcomes, recurrence, or morbidity [38]. On the other hand, LSR was found to have less improvement in constipation scores and higher recurrence rates than LVMR in a randomized study with a median follow-up of 73 months [39].
Technical notes:
This technique requires mobilization of the rectum that varies from limited posterior or anterior to circumferential mobilization. It may include unilateral or bilateral division of the lateral rectal ligaments. After the required mobilization is achieved, the rectum is lifted toward the abdominal wall, and permanent sutures are secured to the right and left sides of the sacral promontory. The sites of sutures should be determined as lateral to hypogastric nerves and medial to ureters [40].
2.1.4. Frykman-Goldberg Procedure (Resection Rectopexy)
In addition to rectopexy, sigmoid resection has been considered effective in terms of recurrence and functional outcomes, particularly in patients with complaints of constipation [14,15,26]. For patients with the main symptom of fecal incontinence, this procedure seems to be unnecessary [41].
Laparoscopic resection rectopexy (LRR) is the most commonly chosen technique for rectal prolapse in the United States [42]. Ashari et al. demonstrated similar improvement rates of continence and constipation (62% and 69%, respectively) and a recurrence rate of 3% with a median follow-up of 62 months [43]. Moreover, a retrospective comparative study between LRR and LVMR reported no significant differences in recurrence and functional outcomes, but higher complication rates in the LRR group [44].
Technical notes:
In this combined procedure, the initial step is complete rectal mobilization; then, the sutures are placed prior to sigmoid resection and tied after colorectal anastomosis. This technique is considered as an optimal treatment for patients with redundant sigmoid and rectal prolapse.
2.1.5. Ventral Mesh Rectopexy
Ventral mesh rectopexy was first described by D’Hoore in 2004 [45]. The main advantage of this technique is the limited dissection anteriorly to the rectum, which enables reinforcement of the rectovaginal septum, preservation of the autonomic nerves, and concomitant colpopexy. High improvement rates in constipation and decreased de novo constipation compared to posterior rectopexy are attributed to the avoidance of complete rectal mobilization [46,47]. Based on these favorable outcomes, ventral mesh rectopexy has become a standard treatment for complete rectal prolapse in European countries [48,49].
This technique has been widely performed via the laparoscopic approach. Randall et al. reported outcomes of 190 patients in a prospective study; recurrence and morbidity rates were 3% and 6%, respectively [50]. In a recent prospective study with a median follow-up of 49 months, improvement in constipation scores was 75%, and there was no reported de novo constipation [51]. Moreover, a systematic review demonstrated that LVMR has the lowest recurrence and morbidity rates with the highest improvement rates in constipation, compared to other laparoscopic rectopexy methods [13].
Lobb et al. reviewed recurrence rates following suture rectopexy and ventral mesh rectopexy in the complete rectal prolapse [52]. A total of 976 patients were included for the suture rectopexy group and 1605 patients for the ventral mesh rectopexy group. Recurrence rates were found to be significantly lower in the ventral mesh rectopexy group; however, it was not statistically confirmed by meta-analysis. Also, subgroup analysis for the type of mesh used in ventral mesh rectopexy (biological vs. synthetic mesh) revealed no difference in terms of recurrence.
Technical notes:
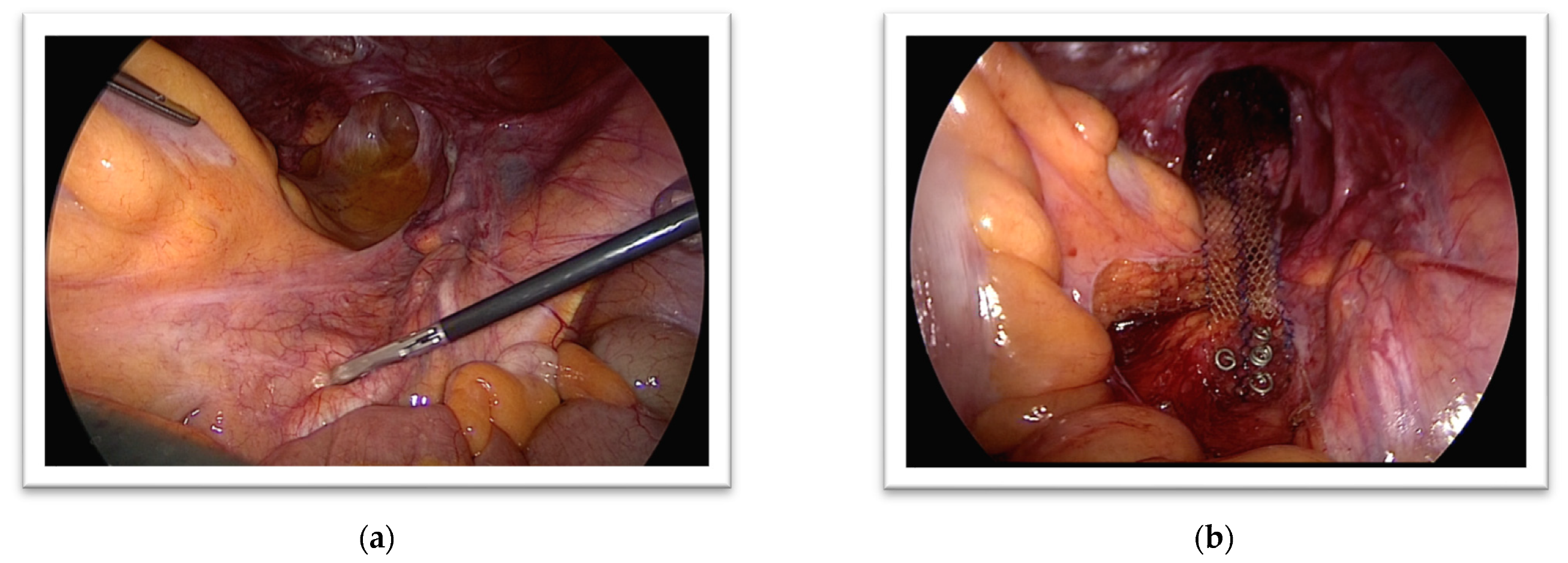
This technique starts with the opening of the peritoneum on the level of promontory and continues laterally to the rectum. The dissection is carried out in Denonvillier’s fascia down to the pelvic floor, and then a mesh reaching up to the promontorium is placed anteriorly to the rectum. Fixation of the mesh can be done with sutures, staples, or surgical glue (Figure 1).
2.2. Perineal Approach
2.2.1. Delorme Mucosectomy
Delorme procedure was first described in 1900 [53], and it is usually preferred in patients with short segments of rectal prolapse [54]. Initial studies reported that this procedure was associated with high recurrence rates and worse functional outcomes [55]. Marchal et al. demonstrated an improvement rate of 42% and 54% of continence and constipation, respectively, and 20% morbidity in patients with a mean follow-up of 73 months [56]. In a prospective study including 113 patients with a mean follow-up of 36 months, an improvement of continence was found to be much higher (89%), with an increased morbidity rate of 30% [57].
On the other hand, Fleming et al. reported similar results between Altemeir and Delorme procedures in terms of functional outcomes, postoperative complications, and mortality [58]. Moreover, in a randomized prospective study comparing patients undergoing Delorme procedure vs. Delorme with levatoroplasty, it was revealed that the combined procedure was associated with decreased recurrence rates and better functional outcomes [59].
Technical notes:
This procedure is performed with the patient in the lithotomy position under regional or general anesthesia. A Lonestar retractor is placed for adequate exposure of the anal verge. A circumferential incision is made in the rectal mucosa 1 cm proximal to the dentate line. The dissection is carried out between the mucosal and muscular layers of the rectum, and a 10–15 cm sleeve of the mucosa is mobilized. Then, the muscle layer of the rectum is longitudinally plicated in four quadrants with 2/0 absorbable sutures. The excess mucosa is excised, and an interrupted mucosal anastomosis is done with 3/0 absorbable sutures [60] (Figure 2).
2.2.2. Altemeier Procedure (Perineal Rectosigmoidectomy)
Altemeier procedure has been commonly performed in patients with long segments of rectal prolapse (>5 cm) [14]. It has also been described as a preferred method for strangulated rectal prolapse combined with diverting ileostomy [61,62]. There are mostly retrospective studies reporting contradicted results regarding functional outcomes, morbidity, and mortality rates of this procedure. In a large retrospective study including 518 patients, morbidity and recurrence rates were 9% and 23%, respectively [63]. On the other hand, Trompetto et al. reported a significantly higher morbidity rate of 38% and recurrence rate of 35% in patients with a median follow-up of 49 months [64].
A comparative study between patients undergoing Altemeir and Delorme procedures revealed no differences regarding morbidity, recurrence rates, and functional outcomes between these two approaches [65]. It has also been recommended that this procedure should be performed in combination with levatoroplasty due to the worsening of fecal incontinence [66].
Technical notes:
The patient is placed in the jack-knife position, and the prolapse is usually exposed by gentle traction downward with Babcock forceps. The dissection site is identified as 2–4 cm proximal to the dentate line and marked with diathermy. The circumferential incision is made, including all the layers of the rectum. First, the extraperitoneal rectum is exteriorized, and then, the dissection is carried out in the rectovaginal septum to open the Douglas pouch. Once the sigmoid colon and rectum are completely mobilized, coloanal anastomosis can be performed with interrupted 3/0 absorbable sutures or a circular stapler [67].
2.2.3. Perineal Stapled Prolapse Resection (PSPR)
PSPR is faster and easier than conventional perineal procedures and it is suitable for high-risk patients under spinal anesthesia. However, high rates of early recurrence have been reported by several studies [68,69]. Tschuor et al. reported a recurrence rate of 44% in a median follow-up of 40 months [70]. Even though the recurrence rates were comparable to Altemeier’s and Delorme’s procedures in a recent meta-analysis, the authors emphasized the necessity of further randomized prospective studies comparing PSPR with other techniques in complete rectal prolapse [71].
Technical notes:
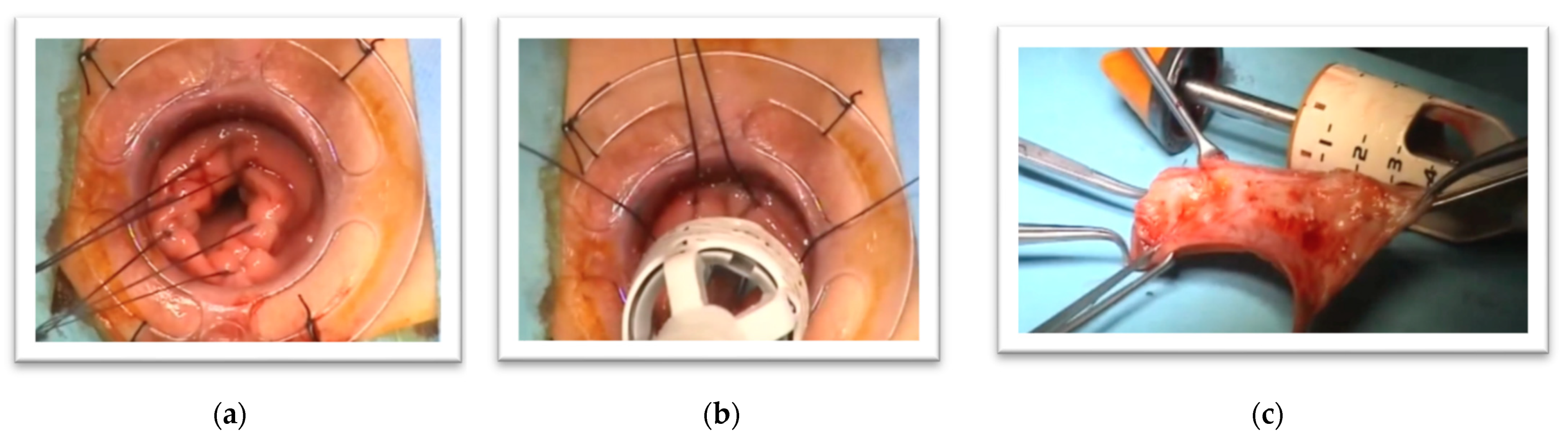
The patient is placed in lithotomy position and adequate exposure is achieved with the anal dilator. The anal dilator is then fixated with sutures to the anal skin. The prolapsed rectum is pulled back with an aid of gauze swab through the anal dilator. Vertical or transverse purse-string sutures are placed 1–2 cm above the dentate line. With traction of these sutures, the prolapsed area is directly visualized, and this provides an accurate position for the stapling device (Figure 3).
3. Conclusions
Complete rectal prolapse is a disabling condition that presents with fecal incontinence, constipation and rectal discharge. Comprehensive diagnostic tests provide clinicians with valuable information by detecting any underlying pathology and suggesting which patient will benefit from which procedure.
This article aimed to review these different procedures for their surgical and functional outcomes. However, the presented studies in this review are quite heterogeneous in terms of the study population, the length of follow-up, the evaluation of recurrence, and the scales to assess incontinence/constipation scores. Ultimately, the best treatment is individualized treatment, and each patient should be treated with an individualized approach based on their prominent symptoms, anatomical deformity, and the surgeon’s experience. The pelvic surgeon should not stick to a single technique, he/she should have all the above-cited techniques in his armamentarium, and the most convenient technique for an individual patient should be decided and performed in a masterly manner.
Author Contributions
Conceptualization, B.M. and S.L.; literature review, B.B. and A.Y.; writing—original draft preparation, B.B. and A.Y.; writing—review and editing, S.L. and B.M.; visualization, S.L.; supervision, S.L. and B.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, due to it being a review article.
Informed Consent Statement
Patient consent was waived due to it being a review article which does not include any patient data.
Data Availability Statement
Present study does not report any new data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lowry, A.C.; Simmang, C.L.; Boulos, P.; Farmer, K.C.; Finan, P.J.; Hyman, N.; Killingback, M.; Lubowski, D.Z.; Moore, R.; Penfold, C.; et al. Consensus statement of definitions for anorectal physiology and rectal cancer. ANZ J. Surg. 2001, 71, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschcowitz, A.V. The pathogenesis, anatomy, and cure of prolapse of the rectum. Dis. Colon Rectum 1983, 26, 553–565. [Google Scholar] [CrossRef]
- Devadhar, D.S.C. A new concept of mechanism and treatment of rectal procidentia. Dis. Colon Rectum 1965, 8, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Engledow, A.; Crosbie, J.; Arulampalam, T.; Motson, R. Laparoscopic nonresectional suture rectopexy in the management of full-thickness rectal prolapse: Substantive retrospective series. Surg. Endosc. 2011, 25, 1062–1064. [Google Scholar] [CrossRef]
- Hawkins, A.; Olariu, A.G.; Savitt, L.R.; Gingipally, S.; Wakamatsu, M.M.; Pulliam, S.; Weinstein, M.M.; Bordeianou, L. Impact of rising grades of internal rectal intussusception on fecal continence and symptoms of constipation. Dis. Colon Rectum 2016, 59, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-S.; Tsang, C.B.S.; Wong, D.W.; Lowry, A.C.; Goldberg, S.M.; Madoff, R.D. Complete rectal prolapse: Evolution of management and results. Dis. Colon Rectum 1999, 42, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Bordeianou, L.; Hicks, C.W.; Kaiser, A.M.; Alavi, K.; Sudan, R.; Wise, P.E. Rectal Prolapse: An overview of clinical features, diagnosis, and patient-specific management strategies. J. Gastrointest. Surg. 2014, 18, 1059–1069. [Google Scholar] [CrossRef]
- Pannu, H.K.; Kaufman, H.S.; Cundiff, G.W.; Genadry, R.; Bluemke, D.A.; Fishman, E.K. Dynamic MR imaging of pelvic organ prolapse: Spectrum of abnormalities. Radiographics 2000, 20, 1567–1582. [Google Scholar] [CrossRef] [Green Version]
- Comiter, C.V.; Vasavada, S.P.; Barbaric, Z.L.; Gousse, A.; Raz, S. Grading pelvic prolapse and pelvic floor relaxation using dynamic magnetic resonance imaging. Urology 1999, 54, 454–457. [Google Scholar] [CrossRef]
- Pucciani, F. Anorectal manometry. In Colon, Rectum and Anus: Anatomic, Physiologic and Diagnostic Bases for Disease Management; Ratto, C., Parello, A., Donisi, L., Litta, F., Eds.; Springer: Cham, Switzerland, 2017; pp. 277–283. [Google Scholar]
- Glasgow, S.; Birnbaum, E.H.; Kodner, I.J.; Fleshman, J.W.; Dietz, D.W. Preoperative anal manometry predicts continence after perineal proctectomy for rectal prolapse. Dis. Colon Rectum 2006, 49, 1052–1058. [Google Scholar] [CrossRef]
- Dvorkin, L.S.; Chan, C.L.H.; Knowles, C.H.; Williams, N.S.; Lunniss, P.J.; Scott, M.S. Anal sphincter morphology in patients with full-thickness rectal prolapse. Dis. Colon Rectum 2004, 47, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Tsunoda, A. Surgical treatment of rectal prolapse in the laparoscopic era; A review of the literature. J. Anus Rectum Colon 2020, 4, 89–99. [Google Scholar] [CrossRef]
- Gallo, G.; Martellucci, J.; Pellino, G.; Ghiselli, R.; Infantino, A.; Pucciani, F.; Trompetto, M. Consensus statement of the Italian Society of Colorectal Surgery (SICCR): Management and treatment of complete rectal prolapse. Tech. Coloproctology 2018, 22, 919–931. [Google Scholar] [CrossRef]
- Tou, S.; Brown, S.R.; Nelson, R.L. Surgery for complete (full-thickness) rectal prolapse in adults. Cochrane Database Syst. Rev. 2015, 2015, CD001758. [Google Scholar] [CrossRef] [PubMed]
- Mustain, W.C.; Davenport, D.L.; Parcells, J.P.; Vargas, H.D.; Hourigan, J.S. Abdominal versus perineal approach for treatment of rectal prolapse: Comparable safety in a propensity-matched cohort. Am. Surg. 2013, 79, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Emile, S.H.; Elbanna, H.; Youssef, M.; Thabet, W.; Omar, W.; Elshobaky, A.; El-Hamed, T.M.A.; Farid, M. Laparoscopic ventral mesh rectopexy vs. Delorme’s operation in management of complete rectal prolapse: A prospective randomized study. Color. Dis. 2017, 19, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Senagore, A.J.; Luchtefeld, M.A. Laparoscopic-assisted vs. open resection. Rectopexy offers excellent results. Dis. Colon Rectum 1995, 38, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.J.; Young, C.J.; Eyers, A.A.; Roberts, R.A. Randomized clinical trial of laparoscopic versus open abdominal rectopexy for rectal prolapse. BJS 2002, 89, 35–39. [Google Scholar] [CrossRef]
- Demirbas, S.; Akin, M.L.; Kalemoglu, M.; Ogün, I.; Celenk, T. Comparison of laparoscopic and open surgery for total rectal prolapse. Surg. Today 2005, 35, 446–452. [Google Scholar] [CrossRef]
- Ripstein, C.B. Treatment of massive rectal prolapse. Am. J. Surg. 1952, 83, 68–71. [Google Scholar] [CrossRef]
- Hrabe, J.; Gurland, B. Optimizing treatment for rectal prolapse. Clin. Colon Rectal Surg. 2016, 29, 271–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tjandra, J.J.; Fazio, V.W.; Church, J.M.; Milsom, J.W.; Oakley, J.R.; Lavery, I.C. Ripstein procedure is an effective treatment for rectal prolapse without constipation. Dis. Colon Rectum 1993, 36, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Faucheron, J.-L.; Voirin, D.; Riboud, R.; Waroquet, P.-A.; Noel, J. Laparoscopic anterior rectopexy to the promontory for full-thickness rectal prolapse in 175 consecutive patients. Dis. Colon Rectum 2012, 55, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Faucheron, J.-L.; Trilling, B.; Girard, E.; Sage, P.-Y.; Barbois, S.; Reche, F. Anterior rectopexy for full-thickness rectal prolapse: Technical and functional results. World J. Gastroenterol. 2015, 21, 5049–5055. [Google Scholar] [CrossRef] [PubMed]
- Sohn, V.; Steele, S.R.; Mellgren, A. Rectopexy with mesh according to the Ripstein technique. In Rectal Prolapse: Diagnosis and Clinical Management; Altomare, D.F., Pucciani, F., Eds.; Springer: Milan, Italy, 2008; pp. 121–129. [Google Scholar]
- Sayfan, J.; Pinho, M.; Alexander-Williams, J.; Keighley, M.R.B. Sutured posterior abdominal rectopexy with sigmoidectomy compared with Marlex® rectopexy for rectal prolapse. Br. J. Surg. 1990, 77, 143–145. [Google Scholar] [CrossRef]
- Dulucq, J.-L.; Wintringer, P.; Mahajna, A. Clinical and functional outcome of laparoscopic posterior rectopexy (Wells) for full-thickness rectal prolapse. A prospective study. Surg. Endosc. 2007, 21, 2226–2230. [Google Scholar] [CrossRef] [PubMed]
- Thejeswi, P. Evaluation of clinical outcomes after abdominal rectopexy and Delorme’s procedure for rectal prolapse: A prospective study. J. Clin. Diagn. Res. 2014, 8, NC04–NC07. [Google Scholar] [CrossRef]
- Dyrberg, D.; Nordentoft, T.; Rosenstock, S. Laparoscopic posterior mesh rectopexy for rectal prolapse is a safe procedure in older patients: A prospective follow-up study. Scand. J. Surg. 2015, 104, 227–232. [Google Scholar] [CrossRef]
- Madbouly, K.M.; Youssef, M. Laparoscopic ventral rectopexy versus laparoscopic wells rectopexy for complete rectal prolapse: Long-term results. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 1–6. [Google Scholar] [CrossRef]
- Zbar, A.P. Mesh rectopexy: The Wells technique. In Rectal Prolapse: Diagnosis and Clinical Management; Altomare, D.F., Pucciani, F., Eds.; Springer: Milan, Italy, 2008; pp. 113–120. [Google Scholar]
- Cutait, D. Sacro-promontory fixation of the rectum for complete rectal prolapse. Proc. R. Soc. Med. 1959, 52, 105. [Google Scholar]
- Gourgiotis, S.; Baratsis, S. Rectal prolapse. Int. J. Color. Dis. 2006, 22, 231–243. [Google Scholar] [CrossRef]
- Aitola, P.T.; Hiltunen, K.-M.; Matikainen, M.J. Functional results of operative treatment of rectal prolapse over an 11-year period: Emphasis on transabdominal approach. Dis. Colon Rectum 1999, 42, 655–660. [Google Scholar] [CrossRef]
- Kellokumpu, I.H.; Vironen, J.; Scheinin, T. Laparoscopic repair of rectal prolapse: A prospective study evaluating surgical outcome and changes in symptoms and bowel function. Surg. Endosc. 2000, 14, 634–640. [Google Scholar] [CrossRef]
- Benoist, S.; Taffinder, N.; Gould, S.; Chang, A.; Darzi, A. Functional results two years after laparoscopic rectopexy. Am. J. Surg. 2001, 182, 168–173. [Google Scholar] [CrossRef]
- Sahoo, M.R.; Thimmegowda, A.K.; Gowda, M.S. A single centre comparative study of laparoscopic mesh rectopexy versus suture rectopexy. J. Minimal Access Surg. 2014, 10, 18–22. [Google Scholar] [CrossRef]
- Hidaka, J.; Elfeki, H.; Duelund-Jakobsen, J.; Laurberg, S.; Lundby, L. Functional outcome after laparoscopic posterior sutured rectopexy versus ventral mesh rectopexy for rectal prolapse: Six-year follow-up of a double-blind, randomized single-center study. EClinicalMedicine 2019, 16, 18–22. [Google Scholar] [CrossRef] [Green Version]
- Bergamaschi, R.; Fealk, M. Surgical treatment of rectal prolapse: Rectopexy without mesh. In Rectal Prolapse: Diagnosis and Clinical Management; Altomare, D.F., Pucciani, F., Eds.; Springer: Milan, Italy, 2008; pp. 107–112. [Google Scholar]
- Hsu, A.; Brand, M.I.; Saclarides, T.J. Laparoscopic rectopexy without resection: A worthwhile treatment for rectal prolapse in patients without prior constipation. Am. Surg. 2007, 73, 858–861. [Google Scholar] [CrossRef]
- Jonkers, H.A.F.; Draaisma, W.A.; Wexner, S.D.; Broeders, I.A.M.J.; Bemelman, W.A.; Lindsey, I.; Consten, E.C.J. Evaluation and surgical treatment of rectal prolapse: An international survey. Color. Dis. 2012, 15, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Ashari, L.H.S.; Lumley, J.W.; Stevenson, A.R.L.; Stitz, R.W. Laparoscopically-assisted resection rectopexy for rectal prolapse: Ten years’ experience. Dis. Colon Rectum 2005, 48, 982–987. [Google Scholar] [CrossRef]
- Jonkers, H.A.F.; Maya, A.; Draaisma, W.A.; Bemelman, W.A.; Broeders, I.A.; Consten, E.C.J.; Wexner, S.D. Laparoscopic resection rectopexy versus laparoscopic ventral rectopexy for complete rectal prolapse. Tech. Coloproctology 2014, 18, 641–646. [Google Scholar] [CrossRef] [PubMed]
- D’Hoore, A.; Cadoni, R.; Penninckx, F. Long-term outcome of laparoscopic ventral rectopexy for total rectal prolapse. BJS 2004, 91, 1500–1505. [Google Scholar] [CrossRef]
- Samaranayake, C.; Luo, C.; Plank, A.W.; Merrie, A.E.H.; Plank, L.; Bissett, I.P. Systematic review on ventral rectopexy for rectal prolapse and intussusception. Color. Dis. 2009, 12, 504–512. [Google Scholar] [CrossRef]
- Boons, P.; Collinson, R.; Cunningham, C.; Lindsey, I. Laparoscopic ventral rectopexy for external rectal prolapse improves constipation and avoids de novo constipation. Color. Dis. 2009, 12, 526–532. [Google Scholar] [CrossRef]
- Gurland, B. Ventral Mesh Rectopexy: Is this the new standard for surgical treatment of pelvic organ prolapse? Dis. Colon Rectum 2014, 57, 1446–1447. [Google Scholar] [CrossRef]
- Panis, Y. Laparoscopic ventral rectopexy: Resection or no resection? That is the question. Tech. Coloproctology 2014, 18, 611–612. [Google Scholar] [CrossRef] [Green Version]
- Randall, J.; Smyth, E.; McCarthy, K.; Dixon, A.R. Outcome of laparoscopic ventral mesh rectopexy for external rectal prolapse. Color. Dis. 2014, 16, 914–919. [Google Scholar] [CrossRef]
- Tsunoda, A.; Takahashi, T.; Matsuda, S.; Oka, N.; Kusanagi, H. Midterm functional outcome after laparoscopic ventral rectopexy for external rectal prolapse. Asian J. Endosc. Surg. 2020, 13, 25–32. [Google Scholar] [CrossRef]
- Lobb, H.S.; Kearsey, C.C.; Ahmed, S.; Rajaganeshan, R. Suture rectopexy versus ventral mesh rectopexy for complete full-thickness rectal prolapse and intussusception: Systematic review and meta-analysis. BJS Open 2021, 5. [Google Scholar] [CrossRef]
- Delorme, R. Sur le traitment des prolapses du rectum totaux pour l’excision de la muscueuse rectale ou rectocolique. Bull. Mem. Soc. Paris 1900, 26, 499–518. [Google Scholar]
- Varma, M.; Rafferty, J.; Buie, W.D. Practice parameters for the management of rectal prolapse. Dis. Colon Rectum 2011, 54, 1339–1346. [Google Scholar] [CrossRef]
- Elagili, F.; Gurland, B.; Liu, X.; Church, J.; Ozuner, G. Comparing perineal repairs for rectal prolapse: Delorme versus Altemeier. Tech. Coloproctology 2015, 19, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Marchal, F.; Bresler, L.; Ayav, A.; Zarnegar, R.; Brunaud, L.; Duchamp, C.; Boissel, P. Long-term results of Delorme’s procedure and orr-loygue rectopexy to treat complete rectal prolapse. Dis. Colon Rectum 2005, 48, 1785–1790. [Google Scholar] [CrossRef]
- Watts, A.M.; Thompson, M.R. Evaluation of Delorme’s procedure as a treatment for full-thickness rectal prolapse. Br. J. Surg. 2000, 87, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Fleming, F.J.; Kim, M.J.; Gunzler, D.; Messing, S.; Monson, J.R.T.; Speranza, J.R. It’s the procedure not the patient: The operative approach is independently associated with an increased risk of complications after rectal prolapse repair. Color. Dis. 2012, 14, 362–368. [Google Scholar] [CrossRef]
- Youssef, M.; Thabet, W.; El Nakeeb, A.; Magdy, A.; Alla, E.A.; El Nabeey, M.A.; Fouda, E.Y.; Omar, W.; Farid, M. Comparative study between Delorme operation with or without postanal repair and levateroplasty in treatment of complete rectal prolapse. Int. J. Surg. 2013, 11, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Binda, G.A.; Serventi, A. Perineal approach to external rectal prolapse: The Delorme procedure. In Rectal Prolapse: Diagnosis and Clinical Management; Altomare, D.F., Pucciani, F., Eds.; Springer: Milan, Italy, 2008; pp. 89–96. [Google Scholar]
- Cernuda, R.B.; Ángel, J.P.; Fernández, N.T.; Sánchez-Farpón, J.H.; Pérez, J.A. Álvarez Perineal rectosigmoidectomy (altemeier procedure) as treatment of strangulated rectal prolapse. J. Gastrointest. Surg. 2016, 20, 2102–2103. [Google Scholar] [CrossRef]
- Voulimeneas, I. Perineal rectosigmoidectomy for gangrenous rectal prolapse. World J. Gastroenterol. 2010, 16, 2689–2691. [Google Scholar] [CrossRef]
- Tiengtianthum, R.; Jensen, C.C.; Goldberg, S.M.; Mellgren, A. Clinical outcomes of perineal proctectomy among patients of advanced age. Dis. Colon Rectum 2014, 57, 1298–1303. [Google Scholar] [CrossRef]
- Trompetto, M.; Tutino, R.; Luc, A.R.; Novelli, E.; Gallo, G.; Clerico, G. Altemeier’s procedure for complete rectal prolapse; outcome and function in 43 consecutive female patients. BMC Surg. 2019, 19, 1. [Google Scholar] [CrossRef]
- Senapati, A.; Gray, R.G.; Middleton, L.J.; Harding, J.; Hills, R.; Armitage, N.C.M.; Buckley, L.; Northover, J.M.A. the PROSPER Collaborative Group PROSPER: A randomised comparison of surgical treatments for rectal prolapse. Color. Dis. 2013, 15, 858–868. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.W.; Pikarsky, A.J.; You, S.Y.; Gervaz, P.; Efron, J.; Weiss, E.; Nogueras, J.J.; Wexner, S.D. Perineal rectosigmoidectomy for rectal prolapse: Role of levatorplasty. Tech. Coloproctology 2004, 8, 3–9. [Google Scholar] [CrossRef]
- Altomare, D.F.; Rinaldi, M. Perineal Approach to External Rectal Prolapse: The Altemeier Procedure. In Rectal Prolapse: Diagnosis and Clinical Management; Altomare, D.F., Pucciani, F., Eds.; Springer: Milan, Italy, 2008; pp. 97–102. [Google Scholar]
- Mistrangelo, M.; Tonello, P.; Contul, R.B.; Arnone, G.; Passera, R.; Grasso, L.; Rapetti, L.; Borroni, R.; Pozzo, M.; Roveroni, M.; et al. Perineal stapled prolapse resection for full-thickness external rectal prolapse: A multicentre prospective study. Color. Dis. 2016, 18, 1094–1100. [Google Scholar] [CrossRef]
- Sehmer, D.; Marti, L.; Wolff, K.; Hetzer, F.H. Midterm results after perineal stapled prolapse resection for external rectal prolapse. Dis. Colon Rectum 2013, 56, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Tschuor, C.; Limani, P.; Nocito, A.; Dindo, D.; Clavien, P.-A.; Hahnloser, D. Perineal stapled prolapse resection for external rectal prolapse: Is it worthwhile in the long-term? Tech. Coloproctology 2013, 17, 537–540. [Google Scholar] [CrossRef] [Green Version]
- Fan, K.; Cao, A.M.; Barto, W.; De Lacavalerie, P. Perineal stapled prolapse resection for external rectal prolapse: A systematic review and meta-analysis. Color. Dis. 2020, 22, 1850–1861. [Google Scholar] [CrossRef]
Figure 1.
Laparoscopic ventral mesh rectopexy: The dissection starts with the opening of the peritoneum on the level of the promontory (a); A polypropylene mesh is placed anteriorly to the rectum and fixated to the sacral promontory (b).
Figure 1.
Laparoscopic ventral mesh rectopexy: The dissection starts with the opening of the peritoneum on the level of the promontory (a); A polypropylene mesh is placed anteriorly to the rectum and fixated to the sacral promontory (b).

Figure 2.
Delorme Mucosectomy: A circumferential incision is made in the rectal mucosa (a); The dissection plane between the mucosal and muscular layers of the rectum (b); The sleeve of the mucosa (c); Mucosal anastomosis (d).
Figure 2.
Delorme Mucosectomy: A circumferential incision is made in the rectal mucosa (a); The dissection plane between the mucosal and muscular layers of the rectum (b); The sleeve of the mucosa (c); Mucosal anastomosis (d).

Figure 3.
Perineal stapled prolapse resection: Sutures are placed on top of the prolapse and used for traction (a); A circular stapling device is inserted and fired (b); The resected specimen of the external rectal prolapse (c).
Figure 3.
Perineal stapled prolapse resection: Sutures are placed on top of the prolapse and used for traction (a); A circular stapling device is inserted and fired (b); The resected specimen of the external rectal prolapse (c).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Leventoglu, S.; Mentes, B.; Balci, B.; Yildiz, A. Surgical Techniques for Rectal Prolapse. Gastroenterol. Insights 2021, 12, 310-318. https://doi.org/10.3390/gastroent12030028
AMA Style
Leventoglu S, Mentes B, Balci B, Yildiz A. Surgical Techniques for Rectal Prolapse. Gastroenterology Insights. 2021; 12(3):310-318. https://doi.org/10.3390/gastroent12030028
Chicago/Turabian StyleLeventoglu, Sezai, Bulent Mentes, Bengi Balci, and Alp Yildiz. 2021. "Surgical Techniques for Rectal Prolapse" Gastroenterology Insights 12, no. 3: 310-318. https://doi.org/10.3390/gastroent12030028