
A Meta-Analysis of the Effects of Comprehensive Sexuality Education Programs on Children and Adolescents
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Selection and Exclusion Criteria for the Literature
2.3. Literature Search and Selection
2.4. Data Evaluation
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Selected Studies
3.2. Characteristics of the Educational Target of Comprehensive Sexuality Education
3.3. Characteristics of Outcome Variables in CSE
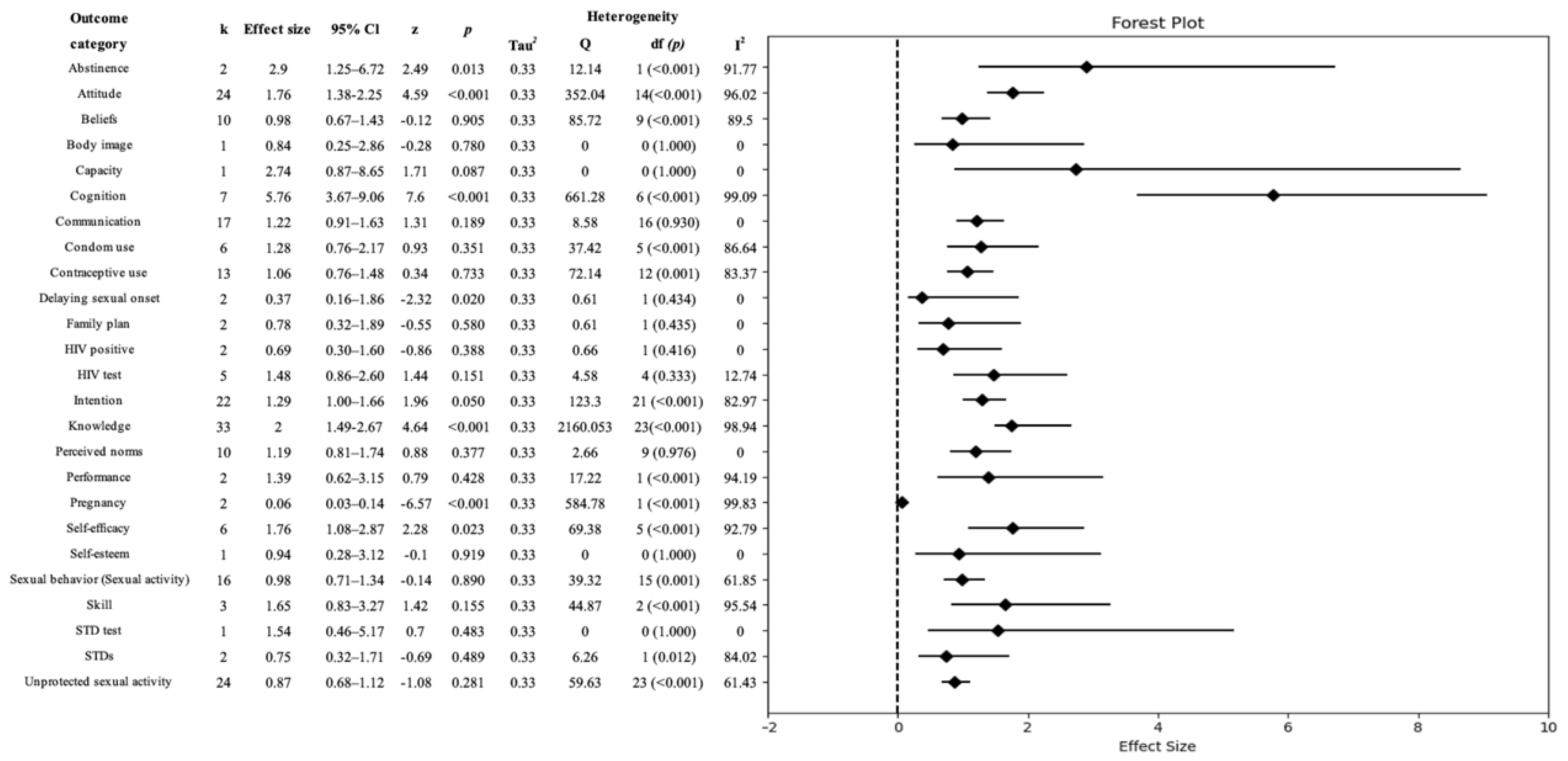
3.4. Effects of Comprehensive Sexuality Education
3.5. Publication Bias in the Meta-Analysis of Comprehensive Sexuality Education
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cacciatore, R.; Korteniemi-Poikela, E.; Kaltiala, R. The steps of sexuality—A developmental, emotion-focused, child-centered model of sexual development and sexuality education from birth to adulthood. Int. J. Sex. Health 2019, 31, 319–338. [Google Scholar] [CrossRef]
- Future of Sex Education Initiative (FOSE). National Sex Education Standards: Core Content and Skills, K-12, 2nd ed.; FOSE: Paris, France, 2020; Available online: https://siecus.org/wp-content/uploads/2020/03/NSES-2020-web-updated-1.pdf (accessed on 28 June 2023).
- Christie, D.; Viner, R. Adolescent development. BMJ 2005, 330, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Hegde, A.; Chandran, S.; Pattnaik, J.I. Understanding adolescent sexuality: A developmental perspective. J. Psychosexual Health 2022, 4, 237–242. [Google Scholar] [CrossRef]
- Widman, L.; Evans, R.; Javidi, H.; Choukas-Bradley, S. Assessment of parent-based interventions for adolescent sexual health: A systematic review and meta-analysis. JAMA Pediatr. 2019, 173, 866–877. [Google Scholar] [CrossRef]
- Molina, A.B.; Rojas Tejada, A.J. Condom use, number of partners and sexual debut in young people in penile-vaginal intercourse, oral sex and anal sex. Rev. Int. Androl. 2018, 16, 8–14. [Google Scholar]
- Gazendam, N.; Cleverley, K.; King, N.; Pickett, W.; Phillips, S.P. Individual and social determinants of early sexual activity: A study of gender-based differences using the 2018 Canadian Health Behaviour in School-aged Children Study (HBSC). PLoS ONE 2020, 15, e0238515. [Google Scholar] [CrossRef]
- Kost, K.; Henshaw, S.; Carlin, L. US Teenage Pregnancies, Births and Abortions: National and State Trends and Trends by Race and Ethnicity; Guttmacher Institute: New York, NY, USA, 2010. [Google Scholar]
- Liang, M.; Simelane, S.; Fillo, G.F.; Chalasani, S.; Weny, K.; Canelos, P.S.; Jenkins, L.; Moller, A.-B.; Chandra-Mouli, V.; Say, L. The state of adolescent sexual and reproductive health. J. Adolesc. Health 2019, 65, S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Kitaw, T.A.; Haile, R.N. Time to First Sexual Experience and Its Determinants among Female Youths in Ethiopia: Survival Analysis Based on EDHS 2016. BioMed Res. Int. 2022, 2022, 5030902. [Google Scholar] [CrossRef] [PubMed]
- Krahé, B.; Tomaszewska, P.; Kuyper, L.; Vanwesenbeeck, I. Prevalence of comprehensive sexuality education among young people in Europe: A review of the evidence from 27 EU countries. Aggress. Violent Behav. 2014, 19, 545–558. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Strengthening the Health Sector Response to Adolescent Health and Development; WHO: Geneva, Switzerland, 2009. Available online: https://apps.who.int/iris/handle/10665/340531 (accessed on 16 June 2023).
- United Nations Educational, Scientific and Cultural Organization (UNESCO). International Technical Guidance on Sexuality Education; UNESCO: Paris, France, 2018. [Google Scholar]
- Van, L.L.; Walsh, K.; Hand, K.; French, S.; Moran, C. Effectiveness of relationships and sex education: A systematic review of terminology, content, pedagogy, and outcomes. Educ. Res. Rev. 2023, 39, 1–24. [Google Scholar]
- Chavula, M.P.; Zulu, J.M.; Hurtig, A.-K. Factors influencing the integration of comprehensive sexuality education into educational systems in low-and middle-income countries: A systematic review. Reprod. Health 2022, 19, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Miedema, E.; Le Mat, M.L.J.; Hague, F. But is it comprehensive? Unpacking the ‘comprehensive’ in comprehensive sexuality education. Health Educ. J. 2020, 79, 747–762. [Google Scholar] [CrossRef]
- Booth, R.E.; Davis, J.M.; Dvoryak, S.; Brewster, J.T.; Lisovska, O.; Strathdee, S.A.; Latkin, C.A. HIV incidence among people who inject drugs (PWIDs) in Ukraine: Results from a clustered randomised trial. Lancet HIV 2016, 3, e482–e489. [Google Scholar] [CrossRef] [PubMed]
- National Evidence-based Healthcare Collaboration Agency (NECA). NECA’s Guidance for Undertaking Systematic Review and Meta-Analyses for Intervention; NECA: Seoul, Republic of Korea, 2011; Available online: http://www.neca.re.kr/org_bbs_download.do?seq=2118&file_name=6517520130215160555.pdf (accessed on 28 July 2023).
- Borenstein, M.; Hedges, L.E.; Higgins, J.P.T.; Rothstein, H.R. Comprehensive Meta-Analysis, Version 4; Biostat, Inc: Atlanta, GA, USA, 2022. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Song, F.; Sheldon, T.A.; Sutton, A.J.; Abrams, K.R.; Jones, D.R. Methods for exploring heterogeneity in meta-analysis. Eval. Health Prof. 2001, 24, 126–151. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M. Research Note: In a meta-analysis, the I2 index does not tell us how much the effect size varies across studies. J. Physiother. 2020, 66, 135–139. [Google Scholar] [CrossRef]
- Borenstein, M.; Higgins, J.P.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Sotton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on metaanalysis. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: West Sussex, UK; Hoboken, NY, USA, 2009; Available online: https://static2.cyberlibris.com/books_upload/300pix/9780470743379.jpg (accessed on 4 July 2023).
- Borenstein, M. Common Mistakes in Meta-Analysis and How to Avoid Them; Biostat, Inc.: Atlanta, GA, NJ, USA, 2019. [Google Scholar]
- Borenstein, M.; Hedges, L.E.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis, 2nd ed.; Wiley: Hoboken, NJ, USA, 2021. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef]
- Higgins, J.P. Commentary: Heterogeneity in meta-analysis should be expected and appropriately quantified. Int. J. Epidemiol. 2008, 37, 1158–1160. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- IntHout, J.; Ioannidis, J.P.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, M.; Odaimi, T.; Demissie, S.; Lee, A.; Farberov, M. A new peer-to-peer educational model to increase knowledge and acceptability of HPV vaccination. J. Adolesc. Health 2018, 62, S105–S106. [Google Scholar] [CrossRef]
- Hong, L.; He, X.; Xue, L.; Guo, L.; Liu, W. Comprehensive Sexuality Education Improves Primary Students’ Explicit and Implicit Attitudes Toward Homosexuality. Int. J. Sex. Health 2022, 34, 503–520. [Google Scholar] [CrossRef]
- DeGue, S.; Niolon, P.H.; Estefan, L.F.; Tracy, A.J.; Le, V.D.; Vivolo-Kantor, A.M.; Little, T.D.; Latzman, N.E.; Tharp, A.; Lang, K.M. Effects of Dating Matters® on sexual violence and sexual harassment outcomes among middle school youth: A cluster-randomized controlled trial. Prev. Sci. 2021, 22, 175–185. [Google Scholar] [CrossRef]
- Hegdahl, H.K.; Musonda, P.; Svanemyr, J.; Zulu, J.M.; Grønvik, T.; Jacobs, C.; Sandøy, I.F. Effects of economic support, comprehensive sexuality education and community dialogue on sexual behaviour: Findings from a cluster-RCT among adolescent girls in rural Zambia. Soc. Sci. Med. 2022, 306, 115125. [Google Scholar] [CrossRef] [PubMed]
- Grossman, J.M.; Tracy, A.J.; Charmaraman, L.; Ceder, I.; Erkut, S. Protective effects of middle school comprehensive sex education with family involvement. J. Sch. Health 2014, 84, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Dulli, L.; Field, S.; Masaba, R.; Ndiritu, J. Addressing broader reproductive health needs of female sex workers through integrated family planning/HIV prevention services: A non-randomized trial of a health-services intervention designed to improve uptake of family planning services in Kenya. PLoS ONE 2019, 14, e0219813. [Google Scholar] [CrossRef]
- Richards, S.D.; Mendelson, E.; Flynn, G.; Messina, L.; Bushley, D.; Halpern, M.; Amesty, S.; Stonbraker, S. Evaluation of a comprehensive sexuality education program in La Romana, Dominican Republic. Int. J. Adolesc. Med. Health 2019, 33, 20190017. [Google Scholar] [CrossRef]
- Boti, N.; Hussen, S.; Shegaze, M.; Shibru, S.; Shibiru, T.; Zerihun, E.; Godana, W.; Abebe, S.; Gebretsadik, W.; Desalegn, N. Effects of comprehensive sexuality education on the comprehensive knowledge and attitude to condom use among first-year students in Arba Minch University: A quasi-experimental study. BMC Res. Notes 2019, 12, 700. [Google Scholar] [CrossRef]
- Chen, M.; Zimmer, C.; Huang, S.; Tian, R.; Yang, B.; Li, M. The effectiveness of an online sexuality education module in promoting sexual knowledge and attitude change: A cluster randomized controlled trial. Health Educ. Res. 2023, 38, 119–138. [Google Scholar] [CrossRef]
- Constantine, N.A.; Jerman, P.; Berglas, N.F.; Angulo-Olaiz, F.; Chou, C.-P.; Rohrbach, L.A. Short-term effects of a rights-based sexuality education curriculum for high-school students: A cluster-randomized trial. BMC Public Health 2015, 15, 293. [Google Scholar] [CrossRef]
- Coyle, K.; Anderson, P.; Laris, B.; Barrett, M.; Unti, T.; Baumler, E. A group randomized trial evaluating high school FLASH, a comprehensive sexual health curriculum. J. Adolesc. Health 2021, 68, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Fein, L.; Beals, T.; Bracho, A.; Broome, M.; Estes, C.M. Evaluation of a Comprehensive Sex Education Program Developed and Implemented by Medical Students [356]. Obstet. Gynecol. 2015, 125, 112S. [Google Scholar] [CrossRef]
- Fikree, F.F.; Abshiro, W.K.; Mai, M.M.; Hagos, K.L.; Asnake, M. The effect of peer education in dispelling myths and misconceptions about long-acting reversible contraception among ethiopian youth. Afr. J. Reprod. Health 2018, 22, 90–99. [Google Scholar] [PubMed]
- George, G.; Beckett, S.; Reddy, T.; Govender, K.; Cawood, C.; Khanyile, D.; Kharsany, A.B. Role of Schooling and Comprehensive Sexuality Education in Reducing HIV and Pregnancy Among Adolescents in South Africa. J. Acquir. Immune Defic. Syndr. 2022, 90, 270. [Google Scholar] [CrossRef]
- Hall, K.S.; Castaño, P.M.; Westhoff, C.L. The influence of oral contraceptive knowledge on oral contraceptive continuation among young women. J. Women’s Health 2014, 23, 596–601. [Google Scholar] [CrossRef]
- Jennings, J.; Howard, S.; Perotte, C. Effects of a school-based sexuality education program on peer educators: The Teen PEP model. Health Educ. Res. 2014, 29, 319–329. [Google Scholar] [CrossRef]
- Kemigisha, E.; Bruce, K.; Ivanova, O.; Leye, E.; Coene, G.; Ruzaaza, G.N.; Ninsiima, A.B.; Mlahagwa, W.; Nyakato, V.N.; Michielsen, K. Evaluation of a school based comprehensive sexuality education program among very young adolescents in rural Uganda. BMC Public Health 2019, 19, 1393. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Chen, W.; Ding, Y.; Chen, J.; Wu, Q.; Tang, W.; Tian, L.; Li, B. Effect of behavioral intervention based on social media to promote HIV/syphilis testing in young men who have sex with men. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2022, 43, 892–897. [Google Scholar] [PubMed]
- Manaseri, H.; Roberts, K.D.; Barker, L.T.; Tom, T. Pono choices: Lessons for school leaders from the evaluation of a teen pregnancy prevention program. J. Sch. Health 2019, 89, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Mellanby, A.R.; Phelps, F.A.; Crichton, N.J.; Tripp, J.H. School sex education: An experimental programme with educational and medical benefit. BMJ 1995, 311, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Menna, T.; Ali, A.; Worku, A. Effects of peer education intervention on HIV/AIDS related sexual behaviors of secondary school students in Addis Ababa, Ethiopia: A quasi-experimental study. Reprod. Health 2015, 12, 1–8. [Google Scholar] [CrossRef]
- Milhausen, R.R.; DiClemente, R.J.; Lang, D.L.; Spitalnick, J.S.; McDermott Sales, J.; Hardin, J.W. Frequency of sex after an intervention to decrease sexual risk-taking among African-American adolescent girls: Results of a randomized, controlled clinical trial. Sex Educ. 2008, 8, 47–57. [Google Scholar] [CrossRef]
- Rijsdijk, L.E.; Bos, A.E.; Ruiter, R.A.; Leerlooijer, J.N.; de Haas, B.; Schaalma, H.P. The World Starts With Me: A multilevel evaluation of a comprehensive sex education programme targeting adolescents in Uganda. BMC Public Health 2011, 11, 334. [Google Scholar] [CrossRef]
- Robinson, B.B.; Uhl, G.; Miner, M.; Bockting, W.O.; Scheltema, K.E.; Rosser, B.R.; Westover, B. Evaluation of a sexual health approach to prevent HIV among low income, urban, primarily African American women: Results of a randomized controlled trial. AIDS Educ. Prev. 2002, 14, 81–96. [Google Scholar] [CrossRef]
- Rotz, D.; Goesling, B.; Manlove, J.; Welti, K.; Trenholm, C. Impacts of a School-Wide, Peer-Led Approach to Sexuality Education: A Matched Comparison Group Design. J. Sch. Health 2018, 88, 549–559. [Google Scholar] [CrossRef]
- Sa, Z.; Tian, L.; Wang, X. Evidence for a Comprehensive Sexuality Education Intervention that Enhances Chinese Adolescents’ Sexual Knowledge and Gender Awareness and Empowers Young Women. Sex. Roles 2021, 85, 357–370. [Google Scholar] [CrossRef]
- Scull, T.M.; Dodson, C.V.; Geller, J.G.; Reeder, L.C.; Stump, K.N. A Media Literacy Education Approach to High School Sexual Health Education: Immediate Effects of Media Aware on Adolescents’ Media, Sexual Health, and Communication Outcomes. J. Youth Adolesc. 2022, 51, 708–723. [Google Scholar] [CrossRef]
- Taylor, M.; Jinabhai, C.; Dlamini, S.; Sathiparsad, R.; Eggers, M.S.; De Vries, H. Effects of a teenage pregnancy prevention program in KwaZulu-Natal, South Africa. Health Care Women Int. 2014, 35, 845–858. [Google Scholar] [CrossRef]
- Yakubu, I.; Garmaroudi, G.; Sadeghi, R.; Tol, A.; Yekaninejad, M.S.; Yidana, A. Assessing the impact of an educational intervention program on sexual abstinence based on the health belief model amongst adolescent girls in Northern Ghana, a cluster randomised control trial. Reprod. Health 2019, 16, 124. [Google Scholar] [CrossRef]
- Ybarra, M.; Goodenow, C.; Rosario, M.; Saewyc, E.; Prescott, T. An mHealth Intervention for Pregnancy Prevention for LGB Teens: An RCT. Pediatrics 2021, 147, e2020013607. [Google Scholar] [CrossRef] [PubMed]
- Ybarra, M.L.; Prescott, T.L.; Phillips, G.L., 2nd; Bull, S.S.; Parsons, J.T.; Mustanski, B. Pilot RCT Results of an mHealth HIV Prevention Program for Sexual Minority Male Adolescents. Pediatrics 2017, 140, e20162999. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Zhu, G.; Jia, B.; Wang, P.; Zhao, T.; Ma, Y.; Dong, B. The Influencing Factors of Comprehensive Sexuality Education Capacity and Its Correlation with Subjective Social Status among Chinese Junior High School Students. Children 2022, 9, 1201. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. [Google Scholar]
- Mark, N.D.E.; Wu, L.L. More comprehensive sex education reduced teen births: Quasi-experimental evidence. Proc. Natl. Acad. Sci. USA 2022, 119, e2113144119. [Google Scholar] [CrossRef]
- Sexuality Information and Education Council of the United States (SIECUS). Guidelines for Comprehensive Sexuality Education, 3rd ed.; SIECUS: Washington, DC, USA, 2021; Available online: https://siecus.org/wp-content/uploads/2018/07/Guidelines-CSE.pdf (accessed on 8 May 2023).
- Kantor, L.M.; Lindberg, L.D.; Tashkandi, Y.; Hirsch, J.S.; Santelli, J.S. Sex education: Broadening the definition of relevant outcomes. J. Adolesc. Health 2021, 68, 7–8. [Google Scholar] [CrossRef]
- Goldfarb, E.S.; Lieberman, L.D. Three decades of research: The case for comprehensive sex education. J. Adolesc. Health 2021, 68, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, K.; McGlashan, H.; Tirumalai, V.; Fenaughty, J.; Veukiso-Ulugia, A. Relationships and sexuality education: Key research informing New Zealand curriculum policy. Health Educ. J. 2022, 81, 134–156. [Google Scholar] [CrossRef]
- Scull, T.M.; Dodson, C.V.; Evans-Paulson, R.; Reeder, L.C.; Geller, J.; Stump, K.N.; Kupersmidt, J.B. Evaluating the mechanisms and long-term effects of a web-based comprehensive sexual health and media literacy education program for young adults attending community college: Study protocol for a three-arm randomized controlled trial. Trials 2022, 23, 521. [Google Scholar] [CrossRef]
- Sedgh, G.; Bearak, J.; Singh, S.; Bankole, A.; Popinchalk, A.; Ganatra, B.; Rossier, C.; Gerdts, C.; Tuncalp, Ö.; Johnson, B.R.; et al. Abortion incidence between 1990 and 2014: Global, regional, and subregional levels and trends. Lancet 2016, 16, 258–267. [Google Scholar] [CrossRef] [PubMed]
- Scull, T.; Malik, C.; Morrison, A.; Keefe, E. Promoting Sexual Health in High School: A Feasibility Study of A Web-based Media Literacy Education Program. J. Health Commun. 2021, 26, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Wiley, D.C.; Plesons, M.; Chandra-Mouli, V.; Ortega, M. Managing sex education controversy deep in the heart of Texas: A case study of the North East Independent School District (NEISD). Am. J. Sex. Educ. 2020, 15, 53–81. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Categories | Subcategories | k | Percentage |
|---|---|---|---|---|
| Year of publication | Before 2000 | - | 1 | 2.9 |
| From 2001 to 2010 | - | 2 | 5.9 | |
| From 2011 to 2020 | - | 21 | 61.8 | |
| From 2021 to 2023 | - | 10 | 29.4 | |
| Country of Publication | North America (n = 17) | USA | 17 | 50.0 |
| South America (n = 1) | Dominican Republic | 1 | 2.9 | |
| Europe (n = 2) | UK | 1 | 2.9 | |
| Norway (Zambia) | 1 | 2.9 | ||
| Asia (n = 5) | China | 5 | 14.7 | |
| Oceania (n = 3) | Ethiopia | 3 | 8.8 | |
| Africa (n = 6) | Ghana | 1 | 2.9 | |
| Kenya | 1 | 2.9 | ||
| South Africa | 2 | 5.9 | ||
| Uganda | 2 | 5.9 | ||
| Study design | Experimental/Cohort study (n = 47) | RCT/experimental study | 20 | 58.8 |
| Quasi-experimental study | 10 | 29.4 | ||
| Others (n = 6) | Mixed methods | 2 | 5.9 | |
| Non-categories | 2 | 5.9 | ||
| Study duration | <1 year | <6 months | 4 | 11.8 |
| 6–11 months | 3 | 8.8 | ||
| 1–2 years | 12–17 months | 9 | 26.5 | |
| 18–24 months | 2 | 5.9 | ||
| 2–3 years | 25–30 months | 1 | 2.9 | |
| 31–36 months | 1 | 2.9 | ||
| 3–4 years | 48 months | 5 | 14.7 | |
| >5 years | 60 months | 1 | 2.9 | |
| 72 months | 1 | 2.9 | ||
| Not described | - | 7 | 20.6 | |
| Funding | Yes | - | 23 | 67.6 |
| No | - | 11 | 32.4 | |
| Component of CSE | A | - | 13 | 38.2 |
| B | - | 9 | 26.5 | |
| C | - | 4 | 11.8 | |
| D | - | 2 | 5.9 | |
| A, B | - | 2 | 5.9 | |
| A, D | - | 3 | 8.8 | |
| B, D | - | 1 | 2.9 | |
| Quality evaluation | RoB | Low | 18 | 85.7 |
| Some concern | 3 | 14.3 | ||
| High | 0 | 0 | ||
| RoBINS-I | Low | 12 | 92.3 | |
| Some concern | 1 | 7.7 | ||
| High | 0 | 0 |
| Characteristics | Categories | Subcategories | k | Percentage |
|---|---|---|---|---|
| Population | Student | Middle and high school students | 15 | 44.1 |
| Elementary school students | 1 | 2.9 | ||
| College students | 1 | 2.9 | ||
| 11–25-year-old school students | 1 | 2.9 | ||
| Adolescents | - | 6 | 17.6 | |
| Sex | Male | 1 | 2.9 | |
| Female | 4 | 11.8 | ||
| Cisgender female Sexual minority | 1 | 2.9 | ||
| Patients | - | 1 | 2.9 | |
| Female sex workers | - | 3 | 8.8 | |
| Age | 10–19 years | - | 26 | 76.5 |
| 13–25 years | - | 1 | 2.9 | |
| 32 years | 1 | 2.9 | ||
| Not described | - | 6 | 17.6 | |
| Race/ethnicity | Asian | Asian | 5 | 5.6 |
| Chinese | 1 | 1.1 | ||
| Japanese | 1 | 1.1 | ||
| American | Asian-American | 1 | 1.1 | |
| American Indian | 5 | 5.6 | ||
| Chicano | 1 | 1.1 | ||
| Hispanic/Latino | 11 | 12.2 | ||
| African American | 9 | 10 | ||
| Hawaiian | 3 | 3.3 | ||
| Alaskan Native | 1 | 1.1 | ||
| Alaska Native Multiracial | 1 | 1.1 | ||
| African | Amhara | 2 | 2.2 | |
| Oromo | 1 | 1.1 | ||
| Ashantis | 1 | 1.1 | ||
| Kenyan | 1 | 1.1 | ||
| South African Asians | 1 | 1.1 | ||
| Ugandan | 2 | 2.2 | ||
| Zambian | 1 | 1.1 | ||
| European | Ukrainian | 1 | 1.1 | |
| Others | White | 11 | 12.2 | |
| Black | 5 | 5.6 | ||
| Others | 6 | 6.7 | ||
| Other Pacific Island | 3 | 3.3 | ||
| Biracial | 1 | 1.1 | ||
| Spanish descent | 1 | 1.1 | ||
| Not described | 14 | 15.6 | ||
| Sex/gender | Female | - | 8 | 23.5 |
| Male | - | 2 | 5.9 | |
| Female/male | - | 24 | 70.6 | |
| Number of enrolled | <1000 | - | 14 | 41.2 |
| 1000–3000 | - | 6 | 17.6 | |
| >3000 | - | 6 | 17.6 | |
| Not described | - | 8 | 23.5 | |
| Number of randomized | <1000 | - | 14 | 41.2 |
| 1000–3000 | - | 6 | 17.6 | |
| >3000 | - | 6 | 17.6 | |
| Not described | - | 8 | 23.5 | |
| Number of analyzed | <1000 | - | 18 | 52.9 |
| 1000–3000 | - | 8 | 23.5 | |
| >3000 | - | 3 | 8.8 | |
| Not described | - | 5 | 14.7 |
| Categories | Outcome Variables | k | Percentage |
|---|---|---|---|
| Abstinence | Abstinence from sex/Abstaining from penile–vaginal sex | 2 | 0.9 |
| Attitude | Attitudes towards using condoms, healthy sexual behavior, homosexuality, gender roles, and CSE | 24 | 10.1 |
| Beliefs | Beliefs about causes of pregnancy, HIV, STIs/Acceptance of gender roles, dating violence, and rape myths | 10 | 4.8 |
| Body image | Body image | 1 | 0.4 |
| Capacity | CSE capacity | 1 | 0.4 |
| Cognition | Risk perception towards HIV, STIs, pregnancy/Perceived susceptibility, severity, barriers, benefits | 7 | 3.1 |
| Communication | Communication with parents, partner, boyfriend, or girlfriend regarding sexual health | 17 | 8.4 |
| Condom use | Inconsistent or consistent condom use | 6 | 3.1 |
| Contraceptive use | Contraceptive use/Currently using birth control | 13 | 5.3 |
| Delaying sexual onset | Delaying vaginal sex (boys and girls) | 2 | 0.9 |
| Family plan | Family planning referrals (male and female)/Married/Cohabiting | 3 | 1.3 |
| HIV positive | HIV-positive/HIV-negative | 2 | 0.9 |
| HIV test | HIV tested/Not HIV tested/Willingness to HCT | 5 | 2.2 |
| Intention | Intention to use a condom, contraception, protection, prevent pregnancy/Intent for bystander intervention | 22 | 9.7 |
| Knowledge | Knowledge of contraceptive methods, sexual, STD testing, causes of STIs, non-causes of HIV, pregnancy, STI prevention | 33 | 14.1 |
| Perceived norms | Perceived community norms regarding contraceptives, condom use, gender equitability, teen sex description, dating violence, gender roles, contraception, protection norms | 10 | 4.4 |
| Performance | Performance behavior to escape and avoid situations where unwanted sex could happen | 2 | 0.9 |
| Pregnancy | Pregnancy since program enrollment/Was or is pregnant/Never been pregnant | 2 | 0.9 |
| Self-efficacy | Self-efficacy towards condom use/Self-efficacy in dealing with coercive sex/Contraception and protection efficacy | 6 | 3.1 |
| Self esteem | Self esteem | 1 | 0.4 |
| Sexual behavior (sexual activity) | Ever had sex/Had vaginal sex/Rights with steady partner/Number of condomless sex acts/Limiting sexual partner only to one | 16 | 8.4 |
| Skill | CSE skill | 3 | 1.3 |
| STD test | Receiving more than one joint testing | 1 | 0.4 |
| STDs | Reported STD symptoms | 2 | 0.9 |
| Unprotected sexual activity | Unprotected sexual activity/More than one sexual partner/Engage in transactional sex/Sexual violence perpetration or victimization/Teen sexual intentions/Unmet contraceptive needs | 24 | 13.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.J.; Park, B.; Kim, S.K.; Park, M.J.; Lee, J.Y.; Jo, A.R.; Kim, M.J.; Shin, H.N. A Meta-Analysis of the Effects of Comprehensive Sexuality Education Programs on Children and Adolescents. Healthcare 2023, 11, 2511. https://doi.org/10.3390/healthcare11182511
Kim EJ, Park B, Kim SK, Park MJ, Lee JY, Jo AR, Kim MJ, Shin HN. A Meta-Analysis of the Effects of Comprehensive Sexuality Education Programs on Children and Adolescents. Healthcare. 2023; 11(18):2511. https://doi.org/10.3390/healthcare11182511
Chicago/Turabian StyleKim, Eun Joo, Bitna Park, Seong Kwang Kim, Min Ju Park, Ju Yeong Lee, A Ra Jo, Min Jae Kim, and Ha Neul Shin. 2023. "A Meta-Analysis of the Effects of Comprehensive Sexuality Education Programs on Children and Adolescents" Healthcare 11, no. 18: 2511. https://doi.org/10.3390/healthcare11182511